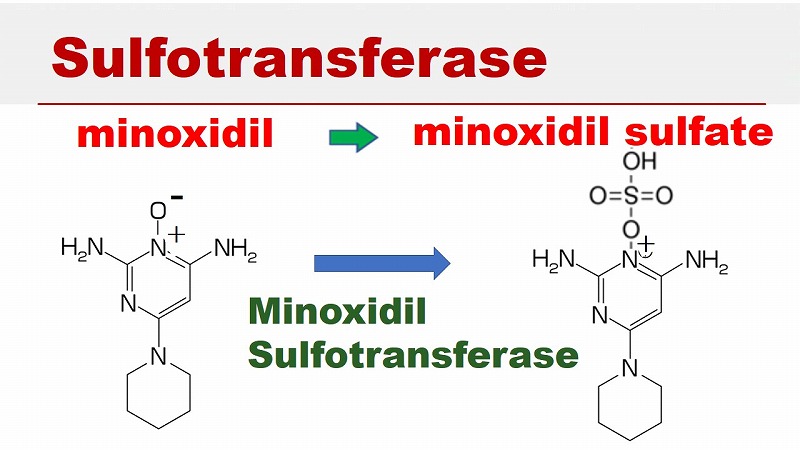
Sulfotransferase & Minoxidil Sulfate
Minoxidil is a pro-drug.
Minoxidil itself does not have any pharmacological effect on hair follicles. Minoxidil doesn’t increase the thickness of hair.
After oral intake or topical application on the scalp, minoxidil is absorbed through the intestine or the skin, and it enters the blood through the capillaries of the intestine or the skin.
Many drugs are absorbed fairly well through the skin.
Minoxidil arrives at the dermal papillae through the systemic blood circulation, and minoxidil is converted into its active form, minoxidil sulfate, by a specific enzyme named sulfotransferase in the outer root sheath of the hair follicles.
Minoxidil sulfate is the active form of minoxidil. Minoxidil sulfate elicits therapeutic responses such as an increase in hair shaft diameter.
Minoxidil sulfate has a clinical effect of making the anagen phase longer and increasing the hair shaft diameter. This is the mechanism how minoxidil makes hair thicker.
As for the effectiveness of minoxidil, it has been reported that hair density increased in 39% of the patients after the treatment with a 5% topical minoxidil solution for 16 weeks. This means that the ratio of responders to a 5% minoxidil solution was about 40% in the population.
The clinical effect of minoxidil depends on the activity of the enzyme sulfotransferase in the outer root sheath of the hair follicles.
There are individual differences in the activity of sulfotransferase, though.
Effects of Minoxidil
Responder vs. Non-Responder

People with good activity of the enzyme sulfotransferase are called “responders”, who can produce more minoxidil sulfate than the others. Hair density increases well in such patients.
The ratio of responders to minoxidil has been reported to be about 40% of the population.
People who respond particularly well to minoxidil can be called “super responders”. They are very lucky people, who can enjoy full volume and density of scalp hair with only topical minoxidil therapy. It is a story only for certain patients.
More than half of the people do not respond to minoxidil very well.
People with less enzyme activity can produce smaller amounts of minoxidil sulfate.
It has been reported that about 60% of the population does not have sufficient activity of sulfotransferase. Minoxidil is less effective than the others in such people.
A person with very poor or no enzyme activity of sulfotransferase is called a “non-responder” to minoxidil. The ratio of non-responders to minoxidil is believed to be about 20% of the population.
Minoxidil is not converted to minoxidil sulfate, and minoxidil does not work effectively in non-responders. Even after the oral or topical minoxidil therapy, hair loss progresses with age in such patients, if predisposition to AGA or diffuse hair loss is superimposed.
With regard to side effects of minoxidil, the risk of systemic side effects of oral minoxidil is much greater than the risk of topical use, by the way.
SULT1A1 gene
minoxidil
The different activity of sulfotransferase is thought to be due to genetic differences.
SULT1A1 gene is involved in the enzyme activity of sulfotransferase.
The SULT1A1 gene encodes minoxidil sulfotransferase (SULT1A1), which is the enzyme that converts minoxidil into its active form of minoxidil sulfate.
Polymorphism of the SULT1A1*2 genotype can cause very low enzyme activity in certain patients found in approximately 20% of the population.
This may explain why the response to minoxidil is low in some specific patients.